1. Lessons Learned: Radiological Protection for Emergency Workers1
1. Introduction
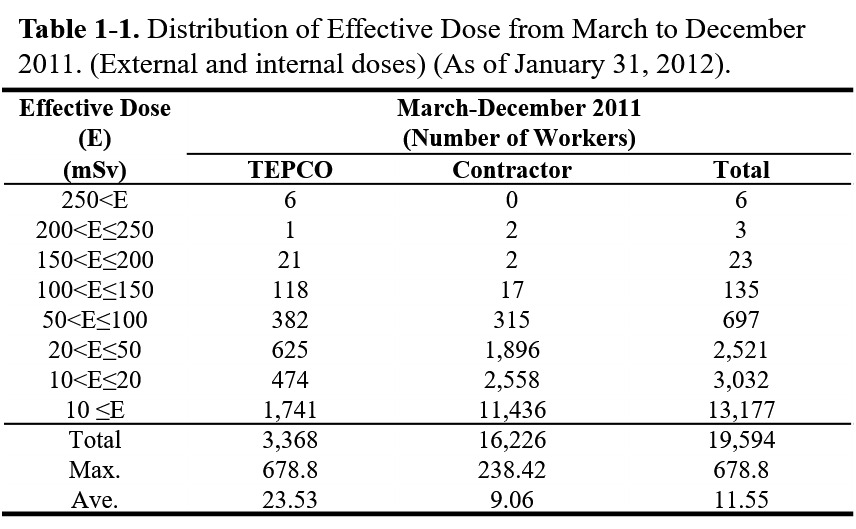
In the response to the Fukushima Daiichi Atomic Power Plant accident that resulted from the East Japan Great Earthquake on March 11, 2011, Tokyo Electric Power Company (TEPCO, hereinafter referred to as “the Company”) undertook emergency work to which the emergency dose limit applied. The Japanese government increased the dose limit to 250 mSv from 100 mSv exclusively for the emergency work performed at the affected plant from March 14 to December 16, 2011. By December 16, 2011, approximately 20,000 emergency workers had been engaged in the work. Their exposure reached a maximum of 678.8 mSv and was 11.55 mSv on average [1] (See Table 1-1).
During the emergency work, the Japanese government experienced various problems. To regulate the implementation of radiological protection for emergency workers, the Ministry of Health, Labour and Welfare issued a series of compulsory directives and provided a number of administrative guidance to the Company.
Based on the experiences and lessons learned, the Ministry recognized that to properly control radiation exposure should a similar accident occur at another atomic power plant, sufficient measures and systematic preparation for radiation control should be ensured, including maintenance of a dosimeter stockpile and implementation of dose data management, personal protective equipment, protective garments, worker training, and work plans.
This article aims to describe lessons learned for practitioner, governmental officials and nuclear operators who are responsible for radiological protection and to provide guidance regarding preparedness for a similar accident.
The article outlines the radiation control problems and exposure reduction problems that occurred during the emergency response to the accident and the response by the Ministry and the Company. Discussion section makes evaluation for the response. To conclude, the recommendations are provided to avoid the recurrence of similar problems.
2. Methodology
On August 10, 2012, the Ministry summarized lessons learned from the accident of the Company Fukushima Daiichi Atomic Power Plant [2] [3] with providing an action timeline, [4] and issued a notification document regarding emergency preparations to all operators of nuclear facilities. [5] Factual information described in this paper was based on the summary and the notification, unless otherwise specified in the references. The author made the best effort to identify references which were available to the public. The observations were also enriched by the personal communications with the Company and relevant experts of the author, who was one of the officers in charge of emergency response to the accident in the Occupational Safety and Health Department of the Ministry.
3. Radiation Control Problems and Response
Prior to the accident, normal operating procedure at the Company controlled access to radiation control areas by checking personal admission cards that displayed personal identification numbers and a photograph. These cards were provided to workers of the Company and contractors. For access to radiation control areas, the Company provided personal dosimeters to all the workers at the entrance to the areas, and a worker was required to register his or her admission card ID number and the dosimeter's serial number at an automatic entrance gate to the controlled area. The electronic dose management system automatically linked the dosimeter data and the ID numbers and printed an individual dose record for each worker when he or she returned the dosimeter at an automatic controlled areas exit gate. The system provided a monthly report of the accumulated external exposure to each worker and a summary report of the external and internal dose every three months, while the whole body counters (WBC: instruments for the measurement of radioactivity within the human body) located in the plant measured the internal exposure of the workers.
On March 11, 2011, the dose management system was nearly destroyed by an earthquake and resulting tsunami, including damage to the electronic dose management system. Moreover, the plant's department of radiation control was occupied with monitoring the ambient dose rate and the radioactive contamination of the rubble and debris caused by the hydrogen explosions of reactors Nos. 1, 3, and 4 and the contaminated water in the basements of the affected reactor and turbine buildings.
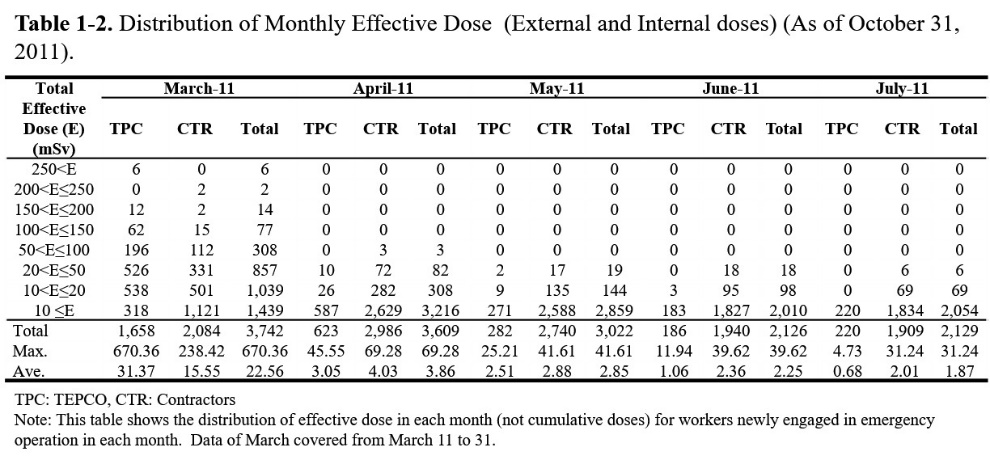
In these circumstances, large numbers of emergency workers were mobilized from other atomic power plants and industrial facilities. The numbers of newly admitted radiation workers were 3,745 in March; 3,620 in April; 3,027 in May; 2,139 in June; and 2,132 in July, which was approximately 3,000 on average until July [6] (Table 1-2). The Company was required to conduct radiation dose control and contamination control for a maximum of approximately 2,800 workers daily. The Company mobilized trained radiation control personnel from other atomic power plants. However, because of the shortage of manpower, equipment, and facilities, the radiation dose management of the emergency workers faced severe challenges.
3.1 Exposure Monitoring and Personal Dosimeters
The tsunami damaged a large number of electronic personal alarm dosimeters. The surviving electric dosimeters could not be recharged because of the electrical blackout at the affected plant. In the response, many dosimeters were sent from other nuclear facilities. However, most of them could not be set to the alarm level because of a lack of calibration equipment. The number of usable dosimeters decreased to approximately 320 on March 15, 2011 [7], whereas the number of emergency workers increased progressively. Under these circumstances, from March 15 to March 31, 2011, the Company implemented a simplified radiation control system that supplied one dosimeter for each work group and regarded the monitored dose as the common dose of the group.
The Company limited the application of the simplified control system to outdoor work, during which the ambient dose is relatively low. However, the group leader's dose could not perfectly represent the dose of a group's individual workers because highly contaminated rubble had scattered across the site during the period.
On March 31, 2011, a shipment of 100 newly purchased electric personal alarm dosimeters arrived and approximately 500 dosimeters arrived from the Company Kashiwazaki-Kariwa atomic power plant so that the total number of dosimeters could reach approximately 920, and on April 1, 2011, the Company recommenced providing dosimeters to all the workers. [7]
3.2 Dosimeter Circulation and Dose Data Management
The Company faced the difficulty of conducting a name-based aggregation of doses and a calculation of accumulated individual doses. In the response to the breakdown of the electronic dose management system, the Company implemented paper-based dosimeter circulation management at the plant until April 4 (until June 8 in the support facility known as J-Village). Workers were required to write down their names and the names of their companies on paper-based dosimeter circulation records. However, there were many cases of improper procedure. For example, certain workers wrote down only their family names, provided illegible language ideograms (in this case, Chinese characters used in Japanese writing), or provided the name of the primary contractor instead of the company that was the worker's employer. In such cases, it was difficult to identify the individual who used a particular dosimeter.
To address these issues, the Company entered the paper-based dose records into a temporary dose management system using personal computers (PCs) and implemented the name-based aggregation of doses using spreadsheet software. In addition, the Company had to manually enter the data and calculate the committed dose of internal exposure, a task that the electronic system had performed automatically prior to the accident. The manpower available for radiation control at the plant was limited, and the number of tasks accumulated. As result, by June 13, 2011 (three months after the accident) the Company had completed only 64% of the name-based dose aggregation for workers in March [8]. Moreover, the PC-based temporary dose management system was unable to print dose records when the workers returned the dosimeters. Therefore, it was difficult for workers to calculate their accumulated doses.
On several occasions after May 23, 2011, the Ministry provided the Company with guidance documents on the improvement of dose management, including the circulation management of the electric dosimeters. In addition, the Ministry required that the Company provide the workers with a printed dose record, when the workers returned their dosimeters. However, the Company could not improve the situation quickly.
The Ministry realized that direct instruction to the primary contractors was indispensable. On July 22, 2011, the Ministry summoned the executive directors of 22 primary contractors and provided guidance from the Director General of the Department of Occupational Safety and Health demanding a full commitment to the dose management of contract workers and requiring that a report on dose distribution be submitted directly to the Ministry.
Following these actions, the Company started to issue worker identification cards on April 4, 2011, for the workers based in the Seismic Isolation Control Building and on June 8, 2011, for the workers based in J-Village in conjunction with the use of personal identification numbers for the dosimeter circulation. However, problems continued, including the duplicate issuance of identification cards for one individual. In addition, the identification cards did not include a photograph, and suspicious cases occurred in which certain workers exchanged identification cards with other workers. In response, beginning July 29, 2011, the Company started issuing worker identification cards with photographs based on the confirmation of worker identity using official documents. In addition, beginning August 8, 2011, the Company initiated the combined use of admission cards with photographs and worker identification cards for access control to reliably verify worker identity.
As for the name-based aggregation, the Company transferred the tasks from the affected plant to the corporate office in Tokyo. However, the name-based aggregation was not started smoothly because the corporate office's radiation control department required time to mobilize sufficient staff. In response, the Company dispatched the number of personnel from other departments and hired new workers and accelerated the name-based aggregation of dose. In cases of unidentifiable data as a result of a missing worker or company name, the Company corrected the data by checking the original paper-based list and making inquiries to the primary contractors. Through these efforts, the Company could obtain an accurate cumulative dose for March 2011 exposures by July 2011. Furthermore, beginning in August 2011, the Company started to provide weekly worker dose records to the primary contractors. Since September 2011, the Company has been able to report the monthly dose distribution to the Ministry by the end of the following month. In addition, since August 16, 2011, the PC-based electronic system has been modified to print a record of the dose when workers return dosimeters.
3.3 Workers Who Were out of Contact
During the process of name-based aggregation, on June 20, 2011, it was revealed that several workers whose identities could not be confirmed appeared on the circular list. When the Company confirmed the identity of these workers and notified the contractors whose names had been provided on the list as employers, several contractors replied that some of these workers were not on their rosters. As the name-based aggregation proceeded, the number of workers who were out of rosters reached 174. It was certain that the workers had engaged in emergency work because there was a dose record data. However, the Company could not determine the workers' identities. This means, for certain workers, the exposure was supposed to be underestimated.
For workers who could not be contacted or identified, the Ministry demanded that the Company assemble an investigation team at the corporate office to investigate the missing workers. In close cooperation with the primary contractors, the Company located the missing workers one-by-one by double-checking the paper-based list, examining data that included a name similar to that of a missing worker, investigation by the primary contractors, and the use of a private investigation firm. As a last resort, the Company released on its website the names of 13 workers who could still not be identified. As a result, three workers reappeared. However, the whereabouts of the others remain unknown.
3.4 Internal Exposure Monitoring
Because of the accident, the Company could not operate the whole body counters (WBC: instruments for the measurement of radioactivity within the human body) that were located in the affected plant because of the increase in the background radiation level. In response, on March 22, 2011, at the Onahama Coal Centre, the Company started to operate two vehicle-mounted whole body counters, which had been borrowed from Japan Atomic Energy Agency (JAEA). However, capacity of the whole body counters was insufficient to cover all of the emergency workers because the total population of emergency workers was increasing monthly by approximately 3,000 workers. In addition, the Company had difficulty coordinating sufficient transportation to Onahama, which is located 50 km from the affected plant.
By June 20, 2011, the Company could not complete the internal exposure monitoring for 125 (3.4%) emergency workers who were engaged in March. This failure was in violation of the Regulation on the Prevention of Ionizing Radiation Hazards, which obligates employers to monitor the internal exposure of workers every three months. [9]
Regarding the delay of internal exposure monitoring, the Ministry issued a document on August 30, 2011, in which the Ministry notified the Company that the Ministry would send the case to the prosecutor's office if the Company failed to correct the violation within one month. The Company succeeded in rectifying the violation. However, six months passed until the Company could conduct monthly internal exposure monitoring for all workers.
The delay was primarily caused by a lack of whole body counters, but there were several related complications. On March 22, 2011, the Company restarted internal exposure monitoring using two vehicle-mounted whole body counters borrowed from the Agency and located at the Onahama Coal Centre 50 km from the affected plant. At that time, many workers had already left the site. In response, the Company stationed another vehicle-mounted whole body counter in Tokyo for the workers who had left. However, because of work schedule adjustments, time was required to bring workers to Tokyo.
For the workers who exhibited a high exposure level after whole body counting in Onahama, it was necessary to conduct additional rounds of monitoring after a 2-week interval following decontamination to eliminate the effect of external contamination. Moreover, workers who required the identification of short-half-life radionuclides, such as I-131, had to be dispatched to the Agency’s Tokai Institute, which was 110 km from the affected plant, to use high-resolution Ge semiconductor detectors because the NaI scintillation detector used in the vehicle-mounted whole body counters had a limited resolution for nuclide identification. This process was time-intensive. Furthermore, the Company dispatched them to the National Institute of Radiological Sciences (NIRS) in Chiba Prefecture, which was 200 km from the affected plant, for internal dose evaluation and a medical check by physicians because workers exposed to more than 100 mSv required medical care. [7] [10]
Additionally, the process of evaluating the committed effective dose (internal exposure dose) from the monitoring results was also time-intensive. Prior to the accident, the Company used an evaluation code based on Co-60. However, this code had to be renewed in accordance with the dominant radionuclides released by the accident: Cs-134, Cs-137, and I-131. Additional time was required to identify the date of the radionuclide intake of the workers, which is indispensable for the evaluation of the internal dose.
Unfortunately, there was no concrete evidence with which to identify the intake date. The Company argued that the intake date should be the middle of the work period at the affected plant, whereas the Ministry insisted that it should be the day of the hydrogen explosion (March 12, 2011) to facilitate a more conservative evaluation. In the end, on June 13, 2011, Dr. Makoto Akashi, an executive director of the National Institute of Radiological Science, made the final decision that the intake date should be March 12, 2011, to facilitate the most conservative evaluation of internal exposure.
On July 10, 2011, the Company opened the WBC Centre in J-Village using relocated usable whole body counters from the affected plant and the Fukushima Daini atomic power plant as well as counters borrowed from the Agency. Using those counters, beginning in September, six months after the accident, the Company could monitor the internal exposure of all the workers monthly. Since October 18, 2011, the Company has been operating a total of 11 counters, including six newly purchased counters.
3.5 Exceeding Emergency Dose Limits
On July 7, 2011, the Institute determined that the doses of six emergency workers had exceeded the emergency dose limit (250 mSv) [11]. The Company entrusted the Institute with the evaluation of the dose as the final step of the internal exposure monitoring of workers suspected of being exposed over the limit. The dose distribution details are shown in Table 1-3 [7].
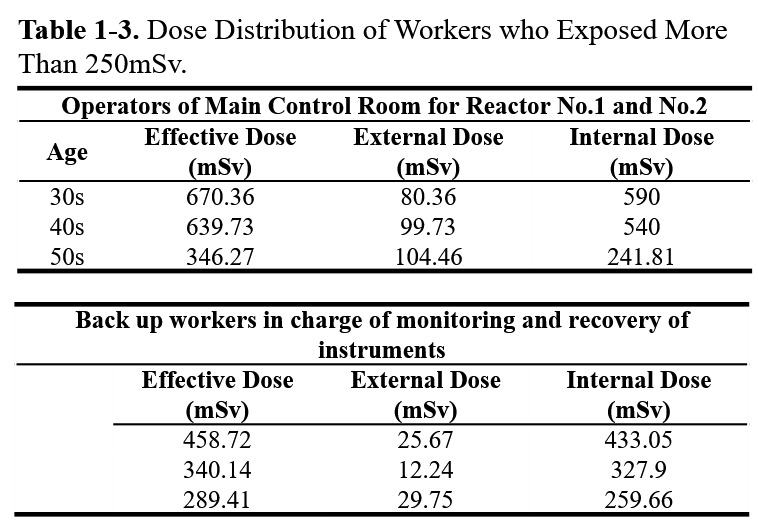
It was beyond the expectations of the Company and the Ministry that several workers in the main control room, who were indoor workers, would exceed the emergency dose limit of 250 mSv. Because the Company gave the first priority for conducting internal exposure monitoring to the workers who were externally exposed to 100 mSv or more, monitoring of indoor workers was delayed. The initial report of this exposure incident was received by the Ministry on May 30, 2011, two and a half months after the accident. To determine the internal dose of these indoor workers, two additional weeks were required for monitoring using Japan Atomic Energy Agency's high resolution Germanium (Ge) semiconductor detectors and bio-assay monitoring by the National Institute of Radiological Science.
The Ministry required the Company to restrict the workers whose tentative internal dose was 100 mSv or more from participating in emergency work until the dose was determined. From the reported provisional assessment of the internal dose, the Ministry was concerned that workers exposed beyond the limit might be found among the workers whose internal dose had not yet been determined. Additionally, the Ministry requested the permanent relocation of those workers whose tentative internal dose was 200 mSv or more from the affected plant.
Following the requests, from June 13, 2011, until the dose was determined, the Company relocated workers suspected of being internally exposed to 100 mSv or more to non-radiation work. In addition, workers suspected of being internally exposed to 200 mSv or more were permanently relocated to other sites. Fortunately, no workers exceeded the dose limits except the main control room staff.
4. Exposure Reduction Problems and Response
4.1 Respiratory Protection
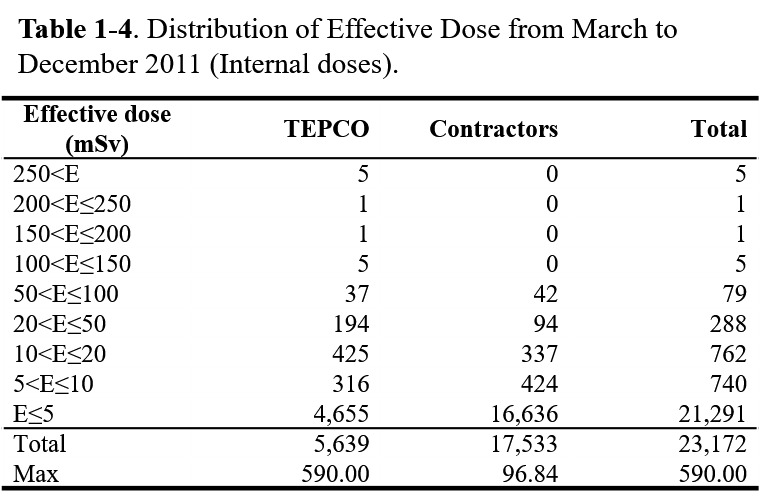
Internal exposure was the most significant influence on radiation control at the affected plant. Twelve workers received more than 100 mSv of internal dose, and five workers exceeded 250 mSv of internal dose (Table 1-4). [12] Internal exposure was preventable had the respirators been properly fitted and the workers followed respiratory protection guidelines for the proper use of respirators. Internal exposures beyond record levels were repeatedly found until September, which was six months after the accident. In addition, inappropriate behavior occurred, such as when a worker failed to attach filters to his mask and when another worker smoked during work after removing his mask.
All cases of internal exposure in excess of the limit occurred in the main control room of reactors No. 3 and No. 4 and the Seismic Isolation Control Building, in which internal exposure was not expected to occur because the ventilation systems are closed. In fact, immediately after the accident, the operators introduced electrical cables from a portable generator located outside the building into the control room through a slightly opened emergency door. A hydrogen explosion occurred on March 12, 2011 under these circumstances. The explosion blast, which contained contaminated radioactive material and gas, smashed the door open and rushed into the room. As a result, the room's air was contaminated. However, the operation staffs did not have a means to monitor the air's radioactivity concentration and failed to don respiratory protection immediately.
The staffs donned respirators when they detected an increase in the ambient dose rate by scintillation counters. However, workers did not use the appropriate charcoal-filter respirator cartridges but rather used particulate-filter cartridges, which are not effective against the radioactive gas of I-131. In addition, operators were required to temporarily remove their respirators to eat and drink in a contaminated environment because they remained in the central control room for approximately 20 hr. The inappropriate use of respiratory protection resulted in most of the workers who remained in the room being internally exposed to more than 100 mSv, and 5 workers exceeded 250 mSv of internal dose. [2] [7]
In Seismic Isolation Control Building, four female workers exceeded the dose limit for women of childbearing age (3 mSv/year). The exposure occurred when the building lost airtightness, which normally prevented the inflow of radioactive material, when the blast of a hydrogen explosion distorted the building's entrance door. However, the Company could not monitor the radioactive concentration of the building's indoor air, which resulted in the delayed recognition by the building's managers that the air was contaminated. Consequently, until the evacuation of all female workers on March 23, 2011, respirators were not used in the building. [2] [7]
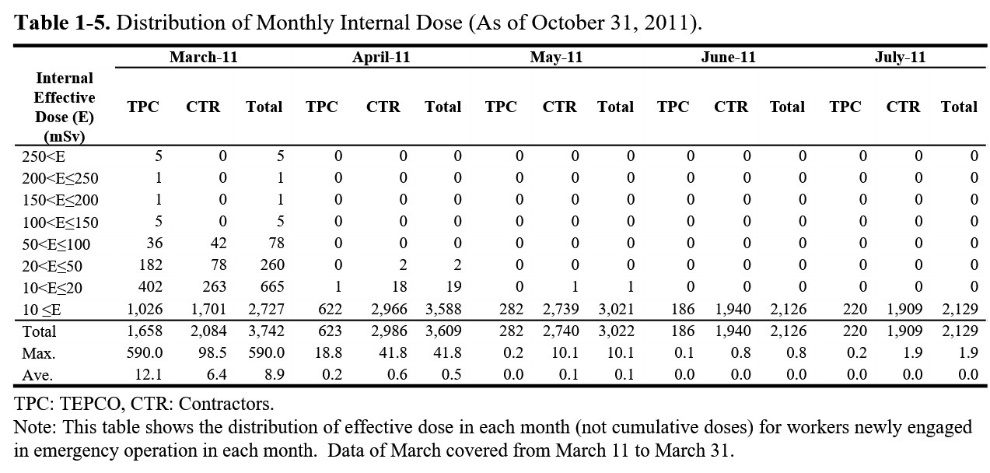
In addition, as late as May 2011, two months after the accident, a worker was observed to have internal exposure of more than 10 mSv. [13] Newly observed internal exposure indicates that respiratory protection was not being used appropriately because internal exposure should not occur if workers are properly fitted for respirators and properly use respiratory protection. (Table 1-5)
Investigation of the proper fitting of respiratory masks
The Ministry decided to investigate the inappropriate use of respiratory protection, including respirator fitting, when the Company reported in September 2011 that significant internal exposure continued to be discovered in workers as late as June 2011. On September 26, 2011, the Ministry conducted an investigation at J-village, the support base located 20 km from the affected plant, jointly with experts from the Japan National Institute of Occupational Safety and Health. In the investigation, the Ministry checked the three types of full-face respirators used at the affected plant and measured leak (filtration) rate of respirators worn by seven the Company workers who performed emergency work during the initial stage of the accident. For the leak test, the Ministry employed a Mask Fitting Tester MT-03 (Shibata Scientific Technology, Ltd. Soka, Saitama, Japan). In addition, the Ministry investigated factors that affected the leakage and evaluated the effectiveness of improvements suggested by experts. [14]
The initial measurement of the leak rate ranged between 1.1% and 56.0% with an average leak rate of 17.4%. The leak rate of workers who wore eyeglasses was higher than other workers. Experts estimated that two main factors affected leakage. The first factor was interference between the respirator face seal and the workers’ faces created by wearing eyeglasses, cotton caps, or workers’ hair interfering with the respirator seal. The second factor was a poor match between the size and shape of the workers’ faces and the size of the respirator.
Based on the expert advice, the leak rate decreased to 5% by applying the following improvements (Table 1-6):
− Attach a pair of seal pieces to the eyeglass frame to fill the gap between the frame and the respirator's face seal.
− Prevent one's cap or hair from interfering with the respirator's face seal.
− Select masks that fit the size and shape of the workers’ faces.

Furthermore, based on the Japan National Institute of Occupational Health’s report released on October 14, 2011, the Ministry requested the Company to implement the following improvements:
− Special measures for eyeglass users, including the attachment of a seal piece to the frame of the eyeglasses.
− Selection of masks which fit the size and shape of the workers’ faces.
− Improvement of respirator fit by the implementation of a leak test.
− Introduction of powered air-purifying respirators (PAPR).
− Improvement of training for new workers regarding the fitting of respirators
After receiving the request, the Company implemented the improvement that, after September 27, 2011, respirators were sorted by size and manufacturer so that workers could choose better-fitting masks. As a consequence, no significant internal exposure was observed after October 2011. However, if the improvements had been introduced earlier, the number of workers exposed internally would be less.
4.2 Protection against Beta-ray Exposure from Contaminated Water
During the emergency work, several incidents of beta-ray exposure occurred in relation to contaminated water. The first incident occurred on March 24, 2011, when workers received beta-ray exposure on their feet after they stepped into 30 cm deep contaminated water while wearing half boots to install electrical cables in a reactor building basement. Investigation revealed that workers did not monitor the ambient dose rate immediately before the work, did not wear long protective boots, and continued to work even after a personal electric dosimeter’s alarm sounded. [15]
Since the contaminated-water processing plant, which filters radioactive cesium from contaminated water, began operation in August 2011, a series of beta-ray exposure incidents have occurred. On August 31, 2011, contaminated water poured over a worker's head as he engaged in draining water from a tank. On the same day, another worker was soaked by contaminated water during the field curing of hoses from the plant. Both workers did not wear liquid-proof coveralls. [2]
An additional beta-exposure incident occurred when three workers directly touched or were close to radioactive strontium-contaminated filters during an exchange of the filters at the contaminated-water processing plant on August 28, 2011. [4]
To prevent the recurrence of the series of beta-ray exposure incidents by contaminated water, the Ministry requested the Company to implement the following improvements:
− Monitor the ambient dose rate of the work sites prior to the work, develop a work plan in consideration of the work sites contamination and undertake tasks following the plan.
− Comply with an evacuation protocol based on dosimeter alarms.
− Use proper protective garments and shoes based on the degree of contamination.
Following the request, the Company fully enforced the use of rubber boots at all times and wearing liquid-proof coveralls when workers handled contaminated water. No incident has occurred since the improvements were introduced.
However, the beta-ray exposure incident that occurred on August 28, 2011 was problematic from the perspective of radiation control. In the affected plant, gamma-ray nucleoli, such as Cs-134 or Cs-137, were dominant in most areas. However, it was revealed that Sr-90, which is a beta-ray-emitting nucleolus, appeared predominantly on the desalination filtration filters for treated water after the contaminated-water processing plant removed Cs-134 or Cs-137 from contaminated water. The monitored 70-μm dose (beta-ray exposure) was 17.1 mSv and 23.4 mSv, whereas the monitored 1-cm dose (gamma-ray exposure) was 0.28 mSv and 0.22 mSv.
According to Radiation Council of Japan guidelines, when beta-ray exposure is more than 10 times gamma-ray exposure, the equivalent dose of extremity should be monitored by ring badges (ring-shaped dosimeters attached to fingers for monitoring skin exposure) and converted to effective dose using tissue weighting factors (0.01 for skin exposure). [16] However, in the affected plant, the Company required workers to wear electric personal alarm dosimeters on their chest, dosimeters which can monitor the 1-cm dose (dose equivalent at a depth of 1 cm point on the human body) and the 70-μm dose (dose equivalent at the skin), but not ring badges. Because the exchange of the filters in August 2011 was a novel experience.
On September 1, 2011, the Ministry required the Company to prevent the recurrence of the incident. After receiving the request, the Company introduced a temporary preventative measure that involved attaching glass badges (radiophoto luminescence (RPL) type passive dosimeters, normally attached on workers’ chests) to the wrists of workers because the Company did not have a sufficient stock of ring badges at the affected plant at that time. Currently, the Company uses ring badges for all workers who handle water contaminated by beta-ray emitting nucleoli.
4.3 Exposure Reduction by Preliminary Review of Work Plan
From March to May 2011, the monthly average dose reached 13.7 mSv, 3.32 mSv, and 2.74 mSv, respectively, [6] which is much higher than the average of other atomic power plants (approximately 1 mSv/year). To reduce radiation exposure, the Ministry requested that the Company submit work plans to the Tomioka Labour Inspection Office, which has authority over the affected plant, prior to work if the exposure was expected to exceed 1 mSv per day. The Ministry started a preliminary review of the plan and provided individual assessments of each plan since May 23, 2011. In the assessments, inappropriate plans appeared repeatedly, e.g., ambient dose rate monitoring was disregarded and exposure reduction was inadequately considered.
Since the preliminary review of work plans started on May 23, 2011, the Company and the primary contractors have submitted approximately 100 work plans to the Tomioka Labour Inspection Office until the end of June, 2011. In the reviews, the Ministry noted inappropriate dose planning as follows:
− A lack of identification of the work sites and insufficient monitoring of the sites' ambient dose rate;
− A lack of care regarding the planned dose—for instance, a maximum planned dose was set at 200 mSv.
In addition, the Ministry observed the inappropriate use of dosimeters such as:
− A lack of external exposure monitoring during standby in the Seismic Isolation Control Building; and
− An excessively high electric dosimeter alarm level, e.g., 10 mSv.
Furthermore, the Ministry noted insufficient deliberation concerning the reduction of exposure—for example,
− Ill-defined work processes;
− The inadequate planning of field working hours; and
− A lack of consideration of radiation shielding.
Additionally, the Ministry noted inadequate evacuation plans, such as the lack of identification of an evacuation route and an evacuation area in case of emergency, including an after quake. [2]
Ambient dose monitoring
One of the most significant problems in developing work plans is the insufficient monitoring of the ambient dose rate, which is indispensable for dose planning. The reasons for insufficient monitoring include:
− The difficulty of identifying the high-dose areas because the highly contaminated rubble of the reactor buildings was scattered by hydrogen explosions;
− A limitation on the number of monitoring points to prevent the excessive exposure of monitoring personnel; and
− The fluctuation of the dose rate after the removal of rubble that shielded other highly contaminated rubble.
Despite these circumstances, the Company and the primary contractors had to commence the emergency work without sufficient monitoring of the ambient dose rate of the working area, solely depending on the alarm of electric dosimeters. As a result, during the emergency work, worker exposures were relatively high. After the cleanup of the rubble was completed in November 2011, the average dose was reduced to approximately 1 mSv per month.
Use of passive dosimeters
Under normal operation, in atomic power plants, regulations oblige workers to wear dosimeters when they engage in radiological work in a control area because radiation exposure is expected to occur solely in control areas. [9] However, in the affected plant, the ambient dose rate in the Seismic Isolation Control Building exceeded 2.5 μSv/hr, which is equivalent to the standard for defining a control area. In addition, radiation exposure during transportation from J-village to the affected plant was not negligible, however, the Company could not monitor the exposure during standby and rest periods in the building because the Company retrieved the dosimeters when the workers returned from their duties. The dosimeters provided by the Company were battery-operated and could not function for more than 13 hr consecutively.
The Ministry requested the Company and primary contractors to use not only electric personal dosimeters but also passive dosimeters such as radiophoto luminescence (RPL) dosimeters or optically stimulated luminescence (OSL) dosimeters on the occasion of a preliminary review of submitted work plans. Eventually, the Company and nearly all of the contractors started to use passive dosimeters and have been able to monitor exposure during standby since November 2011. The radiation dose during standby prior to November was calculated using the ambient dose rate and the number of hours of standby. This exposure was added to the dose monitored by electric dosimeters.
Radiation Exposure Reduction
To decrease radiation exposure, the Company progressively introduced improvements, such as limits on working hours and the use of radiation shielding. In addition, the efforts made to reduce the ambient dose included as following:
− The removal of surface soil, the use of asphalt pavement and steel-panel pavement along the transportation route and at bus stops;
− The closure of windows and the placement of tungsten panels inside the walls of the Seismic Isolation Control Building; and
− Steel-panel pavement on highly contaminated areas of reactor buildings.
In addition, measures adopted for exposure reduction included:
− Wearing tungsten vests in high dose rate areas; and
− The use of remote-controlled construction vehicles.
Furthermore, effective on-site dose control was implemented, such as:
− Standing by in a shielded area;
− The real-time dose monitoring; and
− The prompt rotation of workers when work was performed under high ambient dose rate conditions.
4.4 Worker Training
From the time of the accident until May 2011, the Company and the primary contractors conducted training for newcomers to the affected plant for only 30 min. Eventually, the Company acquired an exclusive classroom for education and started to implement compulsory 7-hr training courses in the summer of 2011, 5 months after the accident.
In Japan, the regulations oblige employers to conduct special education for workers who are engaged in radiological work in control areas. The employer shall provide special training to the said workers on the topics itemized below for a total of 7 hr. [9]
− Knowledge regarding nuclear fuel, spent fuel, or any object contaminated by such material (30 min).
− Knowledge regarding nuclear reactor facility work methods (1 hr and 30 min).
− Knowledge regarding nuclear reactor facility equipment structure and handling methods (1 hr and 30 min).
− Effects of ionizing radiation on human bodies (30 min).
− Related laws and ordinances (1 hr).
− Nuclear reactor facility work methods and the handling of equipment used at such facilities (2 hr).
Immediately after the accident, the training program was completely overwhelmed. In the early stage of the accident, approximately 3,000 new workers required training every month. However, the overpopulated J-village did not possess sufficient space for education and could provide trainings to 20 workers at a time. In response, the Company and the primary contractors conducted simplified, 30-min training courses. It is assumed that insufficient training was one cause of the inappropriate use of masks and protective garments.
On May 13, May 23, and July 22, 2011, the Ministry requested the Company and the primary contractors to conduct training courses for new workers regarding the following:
− The health effects of radiation exposure;
− The use of personal protective equipment; and
− Emergency response.
In response, beginning May 19, 2011, the Company started to conduct special training at its corporate office in Tokyo for workers dispatched to the affected plant. the Company secured an exclusive space for education at J-village and commenced 7-hr compulsory special education for new workers on June 8, 2011, which was 3 months after the accident.
5. Discussion
The Ministry's response to the accident was not in an expeditious manner. Based on the Japanese government's March 14, 2011, decision to increase the emergency dose limit from 100 mSv to 250 mSv, the government had prioritized blocking the spread of the damage from the accident, placing less emphasis on the radiation protection of the emergency workers.
In addition, the Ministry's Tomioka Labour Inspection Office, which had jurisdiction over the affected plant, was largely unable to function during March 2011. Because the office was located in the evacuation area, the Ministry was forced to abandon the office and temporally relocated the office to the meeting room of the Iwaki Labour Inspection Office, which is located 50 kilometers from the affected plant. Moreover, most of the office staff had to evacuate their homes and were living in shelters. In these circumstances, the Ministry could not conduct labor inspections at the affected plant during the accident's early stage.
Furthermore, the Ministry could not obtain information on inappropriate exposure monitoring in March 2011 until the mass media reported the issue. Because there was no direct route of communication to the Company, the Ministry had to gather information regarding the radiation exposure of the emergency workers through the Emergency Response Centre set up in the Cabinet Office.
In April, the Ministry still could not enter the affected plant and could not obtain sufficient information on the radiation protection for the emergency workers. To address the situation, Minister Hosokawa, who was highly concerned regarding the radiation exposure of emergency workers resulting from the increase of the emergency dose limit, decided to visit the affected plant by himself. Before the minister's visit on May 7, 2011, the Ministry performed the first inspection since the accident at J-Village, on May 2, 2011.
J-Village was originally donated by the Company as a contribution to the local economy and had been used as the National Training Centre of the Japan Football Association. The village was located 20 kilometers from the affected plant on the border of the government-designated evacuation area. The facility has many soccer fields and large lodging and meeting facilities. the Company leased J-Village to use as a support facility for the emergency workers, where the Company conducted a surface contamination survey, circulated dosimeters, and supplied personal protective equipment, such as respiratory protection and HAZMAT garments, for the emergency workers. Because, in the affected plant, the Seismic Isolation Emergency Control Building, which was the only building after the accident that was suitable for housing, did not provide sufficient space for radiation control and emergency worker accommodation.
In the May 2, 2011, J-Village inspection, the Ministry confirmed that the Company had used a paper-based circulation list of electronic dosimeters, had a backlog of dose data, and had delayed internal exposure monitoring. As a consequence of Minister Hosokowa's visit to the affected plant, the first labor inspection of the affected plant was conducted on May 27, 2011. The Ministry performed successive inspections on a timely basis later on.
Based on the inspection results, the Ministry decided to require the Company to comply with the following guidance:
− Implement consolidated administrative control over dose data, such as data entry and the name-based aggregation of dose data by the Company Tokyo corporate office in response to the overloaded radiation control departments of the affected plant.
− Collect personal identification information, such as the names and addresses of the emergency workers, and issue worker identification cards with personal identification numbers for the personal identification of the emergency workers.
− Report the external dose distribution to the Ministry every 10 days and the effective dose distribution, including internal exposure, every month to assess worker exposure.
− Submit to the labor inspection office work plans that include radiation exposure reduction measures for work for which the expected dose is more than 1 mSv per day prior to the work being performed.
During the early stage of the accident, the stabilization of the nuclear reactors was the Company's top priority. To emphasize the importance of dose management and exposure reduction for emergency workers and to secure material and manpower for this task, the Ministry decided to require that top the Company executives implement a comprehensive system of dose management and ask for the reaffirmation of the significance of radiation control.
Based on this determination, the Ministry summoned the Company’s board member, to whom the director general of the Occupational Safety and Health Department of the Ministry presented the administrative guidance document including the previously mentioned four requests on May 23, 2011. The Company board member was requested to implement a proper response to the guidance document and to report the results to the Ministry.
As a consequence of the high-level request, the Company corporate office reported detailed information on worker exposure to the Ministry on a timely basis. The Company's dose management department and the Ministry shared information, establishing lines of communication and gradually rebuilding trust. Although problems remained, the new cooperative relationship between the Company and the Ministry fostered an incremental improvement in radiation control at the affected plant.
5.1. Lessons Learned for Radiation Control and Dose Data Management
The affected plant could not independently perform the task of radiation control. Assistance from the power company's corporate office and off-site support facilities outside the evacuation area were indispensable. An on-site emergency response facility should prioritize directing the disaster response and participate only secondarily in the radiation control of emergency workers. Additionally, the power company should prepare off-site support facilities located outside the expected evacuation area (a 20-km radius from the affected plant) that are capable of radiation control and management operations, such as the training of emergency workers, provision of personal protective equipment, circulation of dosimeters, contamination screening of workers/vehicles and internal exposure monitoring.
Moreover, the power company's corporate office, if it is unaffected by the accident and possesses sufficient manpower and equipment, should take responsibility for the portion of radiation control that can be addressed regardless of location, such as dose data entry and name-based dose aggregation and managing the progress of internal exposure monitoring.
The primary contractors should take the dose management responsibilities of the workers or their sub-contractors. Specifically, the primary contractors should act on their own initiative in verifying the identity and affiliation of workers, managing the internal exposure monitoring and notifying the dose to the workers.
The problems that occurred in the accident would not have occurred or would have remained minor if the Company had compiled an operations manual for dose management, stockpiled personal protective equipment and electric dosimeters, and prepared emergency electronic systems and sufficient number of whole body counters prior to the accident. The stockpiling of equipment and the preparation of systems could be more reliable if plant operators could secure agreements on the immediate transport and relocation of equipment to the affected plant in the case of an accident.
Labour standards authorities must compile an emergency operations manual. It is highly probable that employers’ priorities emergency disaster response over the radiation control of workers. Thus, the labor standards authorities should intervene in emergency operations on a timely basis. The manual should list the necessary interventions to be performed by the authority.
5.2 Lessons Learned for Radiation Exposure Reduction
After the accident, the Ministry repeatedly requested the Company and the primary contractors to reduce the radiation exposure with consideration of the need to avoid disturbing the performance of emergency work. However, most of the requests consisted of stopgap measures, which were conceived and recommended after problems occurred. The Company had to implement improvements using trial and error because of a lack of sufficient preliminary review and examination.
With respect to reducing the radiation exposure, several issues remain to be resolved, such as the development of remote-controlled devices for conducting radiological monitoring. However, the following insights should be shared as lessons learned with operators of other plants.
Internal exposure was completely preventable by the proper fit and use of respiratory protection. Internal exposure that exceeded dose limits occurred in main control rooms and the Seismic Isolation Control Building, where internal exposure was not expected. In consideration of the chaos immediately after the accident, it was not straightforward to recognize the failure of airtightness caused by the hydrogen explosions and apply the necessary countermeasures. However, if there had been well-prepared manuals and a sufficient number of proper respiratory masks, the operators could have responded appropriately. In addition, the incidents of significant internal exposure that occurred after April 2011 were not the result of a shortage of respiratory protection but a question of a proper respirator fit. Delayed internal exposure monitoring resulted in further problems because determining the source of the problem and introducing improvements was also delayed. In the simplified training provided during the emergency, respirator fit should have received top priority.
As for the incidents of beta-ray exposure, the fundamental problem was that the Company failed to use liquid-proof garments when necessary. The essence of the accident is the fight against contaminated water because the tsunami was the accident's primary cause. However, the Company failed to prepare sufficient liquid-proof garments, such as rubber boots and waterproof coveralls, and develop manuals for their use. This failure resulted in beta-ray exposure incidents.
The efforts to reduce external exposure required the solution of a substantial number of problems. However, given the problems that the Ministry perceived during the preliminary review of work plans, the planning of work procedures to reduce external exposure was insufficient. For the effective development of work plans, it is indispensable to establish a system in which radiation control units can review the original plans developed by the construction units from the perspective of exposure reduction. Preliminary review by the Ministry assumed the Company's radiation control responsibility and was able to change the Company's attitude toward work planning. This process would be more have been more effective if the Ministry could have started the reviews earlier than the end of May 2011.
The monitoring of the ambient dose rate of the working area is indispensable for developing work procedures during nuclear emergencies. In the case of the affected plant, monitoring the ambient dose rate, sampling contaminated water, and surveying contaminated rubble required human labor. Therefore, the radiation dose of the radiation control unit was relatively high. The further development of remote-controlled devices to monitor and survey the affected area is an urgent requirement. In addition, if well-designed procedures had been developed prior to the accident, the earlier implementation and deployment of remote-controlled construction vehicles, passive dosimeters, tungsten shielding vests, and shielding of Seismic Isolation Control Building could have been possible.
6. Recommendations
6.1 Radiation Control
Regarding the radiation control, nuclear operators should:
− In the preparation for emergency work, develop a plan to establish a department that can control the radiation dose of all emergency workers in an integrated fashion. The department should be established at the affected plant and, should an accident overwhelm the plant's control capacity, an off-site support facility or a corporate office should participate.
− In preparation for the unfunctional of the dose control system, an emergency operations plan should be established, including the temporary increase in radiation control personnel.
− Stockpile a sufficient number of dry-cell battery electric dosimeters or rechargeable electric dosimeters with a recharger and portable electronic generators that can be used in an emergency.
− Arrange a mutual agreement with other nuclear facilities to provide the affected plant with a sufficient number of electric dosimeters for emergency workers.
The corporate offices of atomic power plant operators should:
− In preparation for the establishment of a radiation control department in a corporate office, compile an implementation plan, including the mobilization of materials and personnel.
− In preparation for the dispatch of radiation control personnel to the affected plant, establish a system that includes a list of the personnel to be dispatched and the training of reserves.
The primary contractors should:
− Develop human resources capable of radiation control, and establish a system of emergency dose management.
− Determine methods to confirm the identity of the sub-contractor emergency workers in a timely manner.
6.2 Dose Data Management
Regarding dose data management, nuclear operators should:
− In preparation for an unfunctional electronic dose management system, establish a backup electronic system that can be installed on mobile PCs, that can issue workers an ID card with a personal identification number and a photograph and that can perform the name-based aggregation of dose records. The back-up system should be able to print a record of daily dose when workers return their electric dosimeters.
− In preparation for the failure of the backup system, develop a form and its use procedure for a paper-based dosimeter circulation list. This list should use the number of the worker's driver's license or personal radiation control notebook (when not applicable, a combination of birth date and name) as a temporary ID number for radiation control.
− Regularly conduct an emergency drill to practice the proper implementation of the actions stated in the two immediately preceding points in the case of an accident.
6.3 Internal Exposure Monitoring
Regarding internal exposure monitoring, nuclear operators should:
− Prepare a facility in which to relocate whole body counters borrowed from other nuclear facilities according to a previously established mutual agreement with other atomic power plant operators.
− Develop a method to evaluate the internal exposure of emergency workers, including the determination of intake date using a behavior survey and an evaluation code applicable to radionuclide released.
The corporate offices of atomic power plant operators should:
− Develop a dose evaluation code applicable to Cs-137/134 and I-131 released from the affected plant in cooperation with specialized institutions, such as Japan Atomic Energy Agency and the National Institute of Radiological Science.
− Arrange by mutual agreement that other nuclear facilities will supply the affected plant with whole body counters, and develop an emergency response plan that includes the relocation of counters to off-site support facilities if counters cannot be set up at the affected plant.
6.4 Prevention of internal exposure, including respiratory protection
Regarding internal exposure prevention, nuclear operators should:
− For the timely monitoring of the ambient dose rate of a workplace in which workers remain or standby in the affected plant, prepare radiation monitoring devices and a working procedure for ambient dose rate monitoring.
− In preparation for the contamination of the workplace, stockpile a sufficient number of respirators and charcoal/dust filters in workplaces and store a sufficient number of supplemental filter cartridges in the Seismic Isolation Control Building.
− Provide training on respirator fitting to all emergency workers—in particular, operators who rarely wear masks and eyeglasses users—and periodically repeated. The training should include the following:
⸱ A respirator leak check using fit-testers;
⸱ Supplemental sealing for eyeglasses that includes the application of a seal piece to the eyeglass frame.
− Provide respiratory masks according to size and manufacturer so that workers can select tight-fitting masks that offer the best fit.
− Introduce powered air-purifying respirators (PAPR).
− Stockpile a sufficient number of protective garments, including rubber boots, splash-tight coveralls, and liquid-proof coveralls.
6.5 Radiation exposure reduction by preliminary review of work plans
Regarding ambient dose rate monitoring, nuclear operators and primary contractors should:
− Identify high-dose points as a basis for dose planning.
− Collect information regarding the ambient dose rate, including a dose-rate map, from nuclear operators.
− Monitor the ambient dose rate immediately before the start of work because the ambient dose rate may change drastically in a short time, particularly in affected reactor buildings
Regarding the reduction of radiation exposure, nuclear operators and primary contractors should:
− Implement effective radiation shielding near high dose sources.
− Wear tungsten vests and reduce field working hours as much as possible.
− Identify transportation routes and use vehicles to reduce exposure during transportation.
− Implement training by using mockups to reduce field working hours under high dose rate conditions.
Regarding protective garments, nuclear operators and primary contractors should:
− Use proper protective garments and shoes in accordance with contamination conditions.
− Use proper liquid-proof coveralls and rubber boots when workers handle contaminated water
Regarding radiation monitoring devices, nuclear operators and primary contractors should:
− Use electric dosimeters that can monitor not only the 1-cm dose but also the 70-μm dose rate when workers handle contaminated water.
− Use ring badges for all workers who handle water contaminated by beta-ray emitting nucleoli.
6.6 Worker Training
Regarding worker training, nuclear operators and primary contractors should:
− Secure an exclusive space for education, produce textbooks and prepare trainers to conduct sufficient education for all new workers in the case of an emergency.
− Develop additional training materials regarding evacuation during an emergency, emergency steps, and radiation control and implement training using the materials with periodical re-education.
Corporate offices of atomic power plant operators should:
− Assist in the development of plant’s training materials.
− Educate a sufficient number of trainers and prepare to dispatch them in an emergency.
7. Conclusion
On August 10, 2012, the Ministry issued a notification document which instructed the director generals of the Prefectural Labour Bureaus to urge nuclear operators to perform the necessary preparation listed in Recommendation to avoid similar problems of radiation control, dose data management and exposure reduction in the case of an accident. [5]
Reference
| [1] |
Tokyo Electric Power Company, "Status of Exposure Dose Evaluation for the Workers at Fukushima Daiichi Nuclear Power Station," 31 January 2012. [Online]. Available: http://www.tepco.co.jp/en/press/corp-com/release/2012/12013106-e.html. |
| [2] |
Ministry of Health, Labor and Welfare, "Future Actions Based on Experience such as Exposure Dose Control at the TEPCO Fukushima Daiichi Nuclear Power Plant," 10 August 2012. [Online]. Available: http://www.mhlw.go.jp/english/topics/2011eq/workers/tepco/rp/pr_120810_a01.pdf. |
| [3] |
Ministry of Health, Labor and Welfare, "Response and Action Taken by the Ministry of Health, Labor and Welfare of Japan on Radiation Protection for Workers Involved in the TEPCO Fukushima Daiichi Nuclear Power Plant Accident," 2 November 2013. [Online]. Available: Tokyo. Available at http://www.mhlw.go.jp/english/topics/2011eq/workers/tepco/rp/irpw.pdf . |
| [4] |
Ministry of Health, Labor and Welfare, "Action Time Line after the Great East Japan Earthquake.," [Online]. Available: http://www.mhlw.go.jp/english/topics/2011eq/workers/tepco/ort/ors_003.html . |
| [5] |
Ministry of Health, Labor and Welfare, "Enhancement of Safety and Health Management Measures of Radiation Works and Emergency Work at Nuclear Facilities . (Labor Standards Bureau Notification No. 0810-1)," 10 August 2012. [Online]. Available: http://www.mhlw.go.jp/english/topics/2011eq/workers/tepco/rp/pr_120810_a02.pdf . |
| [6] |
Tokyo Electric Power Company, "Evaluation Status of Internal Exposure Dose of Emergency Workers," 30 November 2011. [Online]. Available: http://www.tepco.co.jp/en/press/corp-com/release/11113013-e.html. |
| [7] |
National Diet of Japan Fukushima Nuclear Accident Independent Investigation Commission, "Ch.4.4.5 Exposure of Nuclear Power Plant Workers," in Reports of the National Diet of Japan Fukushima Nuclear Accident Independent Investigation Commission, K. Kuroda, Ed., National Diet of Japan, 2012, p. Ch4.100–Ch.4.106. |
| [8] |
Tokyo Electric Power Company:, "Evaluation Status of Site Workers’ Exposure Doses During Emergency Work at Fukushima Daiichi Nuclear Power Station," 13 June 2011. [Online]. Available: http://www.tepco.co.jp/en/press/corp-com/release/11061311-e.html. |
| [9] |
"Ordinance on Prevention of Ionizing Radiation Hazards," Ordinance of Ministry of Labour No. 41, 1972. |
| [10] |
Tokyo Electric Power Company, "The Report on Cause Analysis on Exposure of Radiation Workers Exceeding Dose Limit and Development Of Measures On Recurrence Prevention at Emergency Work in Fukushima Daiichi Nuclear Power Station," 17 June 2011. [Online]. Available: http://www.tepco.co.jp/en/press/corp-com/release/betu11_e/images/110617e23.pdf. |
| [11] |
Tokyo Electric Power Company, "Status of Evaluation Work of TEPCO Employees’ Exposure Dose at Fukushima Daiichi Nuclear Power Station (3rd release)," 7 July 2011. [Online]. Available: http://www.tepco.co.jp/en/press/corp-com/release/11070706-e.html. |
| [12] |
World Health Organization, "Health Risk Assessment From the Nuclear Accident After the 2011 Great East Japan Earthquake and Tsunami Based on a Preliminary Dose Estimation," World Health Organization, Geneva, 2013. |
| [13] |
Tokyo Electric Power Company, "Evaluation Status of Internal Exposure Dose of Emergency Workers.," 30 November 2011. [Online]. Available: http://www.tepco.co.jp/en/press/corp-com/release/11113013-e.html. |
| [14] |
Japan National Institute of Occupational Safety and Health, "Report on the Government-requested Investigation on Respiratory Protective Equipment Fitting at the TEPCO Fukushima Daiichi Nuclear Plant Stabilization Center (J Village)," 14 October 2011. [Online]. Available: http://www.mhlw.go.jp/english/topics/2011eq/workers/tepco/rp/pr_111014_a01.pdf. |
| [15] |
Tokyo Electric Power Company, "Result of the Investigation on Exposure to Radiation of Workers From Cooperative Companies at Unit3 in Fukushima Daiichi Nuclear Power Station.," 25 March 2011. [Online]. Available: http://www.tepco.co.jp/en/press/corp-com/release/11032503-e.html. |
| [16] |
Radiation Council of Japan, "Technical Guidelines on Evaluation of External Exposure and Internal Exposure.," 21 August 2001. [Online]. Available: http://www.nsr.go.jp/archive/mext/b_menu/shingi/housha/sonota/990401.htm. |
1 This chapter is derived in part from articles published in Journal of Occupational and Environmental Hygiene 10(11) pp.D151-D158, 2013 and 10(12) pp.D163-D171, 2013, available online: http://dx.doi.org/10.1080/15459624.2013.832613 and http://dx.doi.org/10.1080/15459624.2013.831988